Transplanted
1
View details
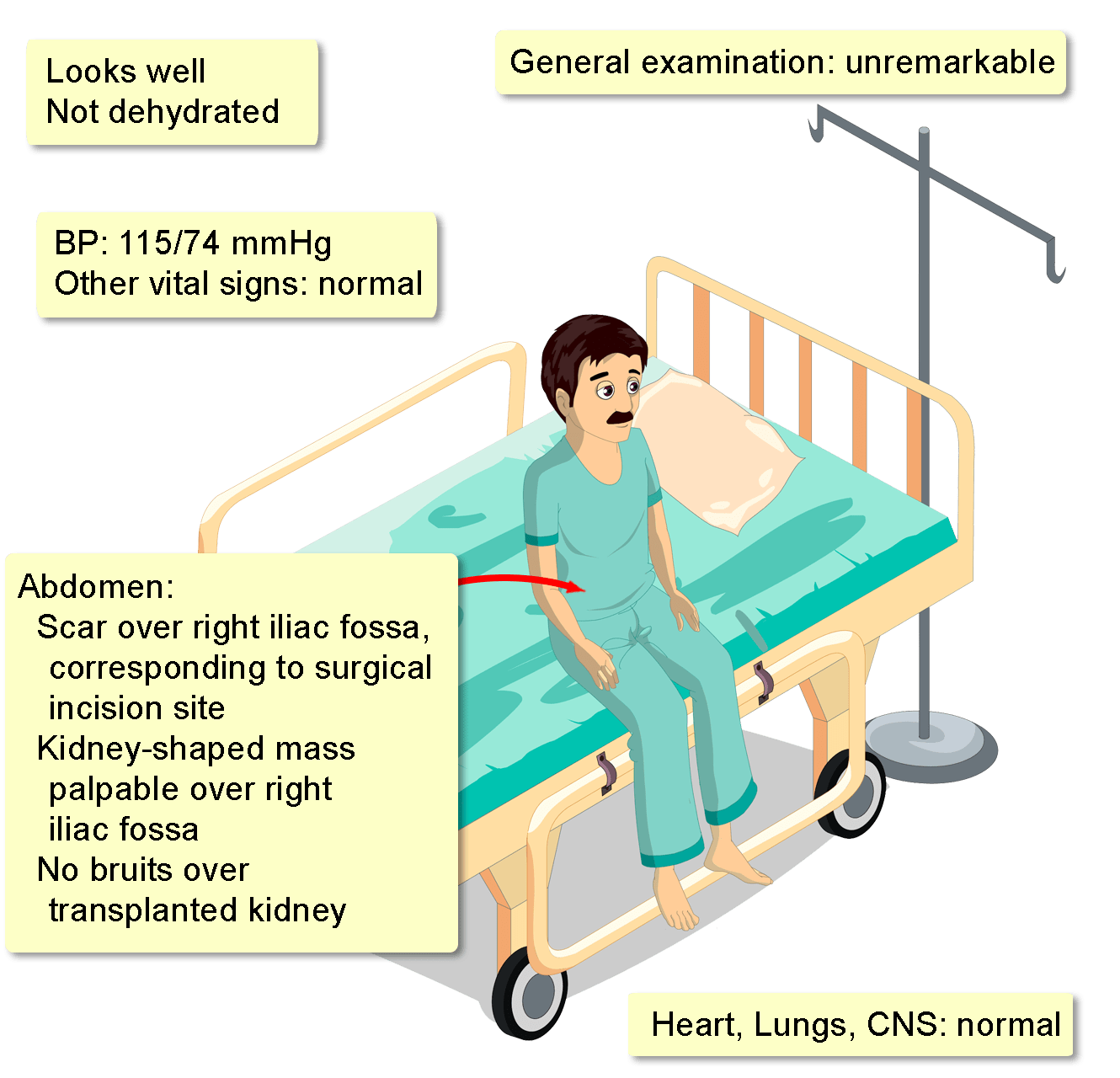
A 35-year-old man who underwent renal transplantation eight months ago is found to have a serum creatinine level of 1.6 mg/dL (normal: 0.6-1.2), during routine follow-up. He is completely asymptomatic, and has maintained a stable weight for the last half-year.
His two most recent clinic visits were six-and-a-half and seven months ago, during which serum creatinine levels were 0.95 mg/dL and 1.0 mg/dL respectively.
He was diagnosed with IgA nephropathy at the age of 23 years, with subsequent progression into bilateral chronic kidney disease and end-stage renal-disease, necessitating deceased-donor kidney transplantation. There were no complications following surgery.
He is currently on maintenance immunotherapy with tacrolimus, mycophenolate mofetil, and prednisone, with excellent compliance.
His medical, surgical, family, and allergic histories are otherwise unremarkable, and he does not smoke, drink, or use recreational drugs.
A complete blood count, electrolyte profile, fasting plasma glucose, and HbA1c are all within normal parameters. Blood urea nitrogen is 13 mg/dL (normal: 7-20).
A urinalysis is also unremarkable, with dipstick testing for both nitrites and leukocyte estate being negative. However, urine cytology demonstrates multiple cells with large homogenous basophilic nuclear inclusions.